Scene 1 (0s)
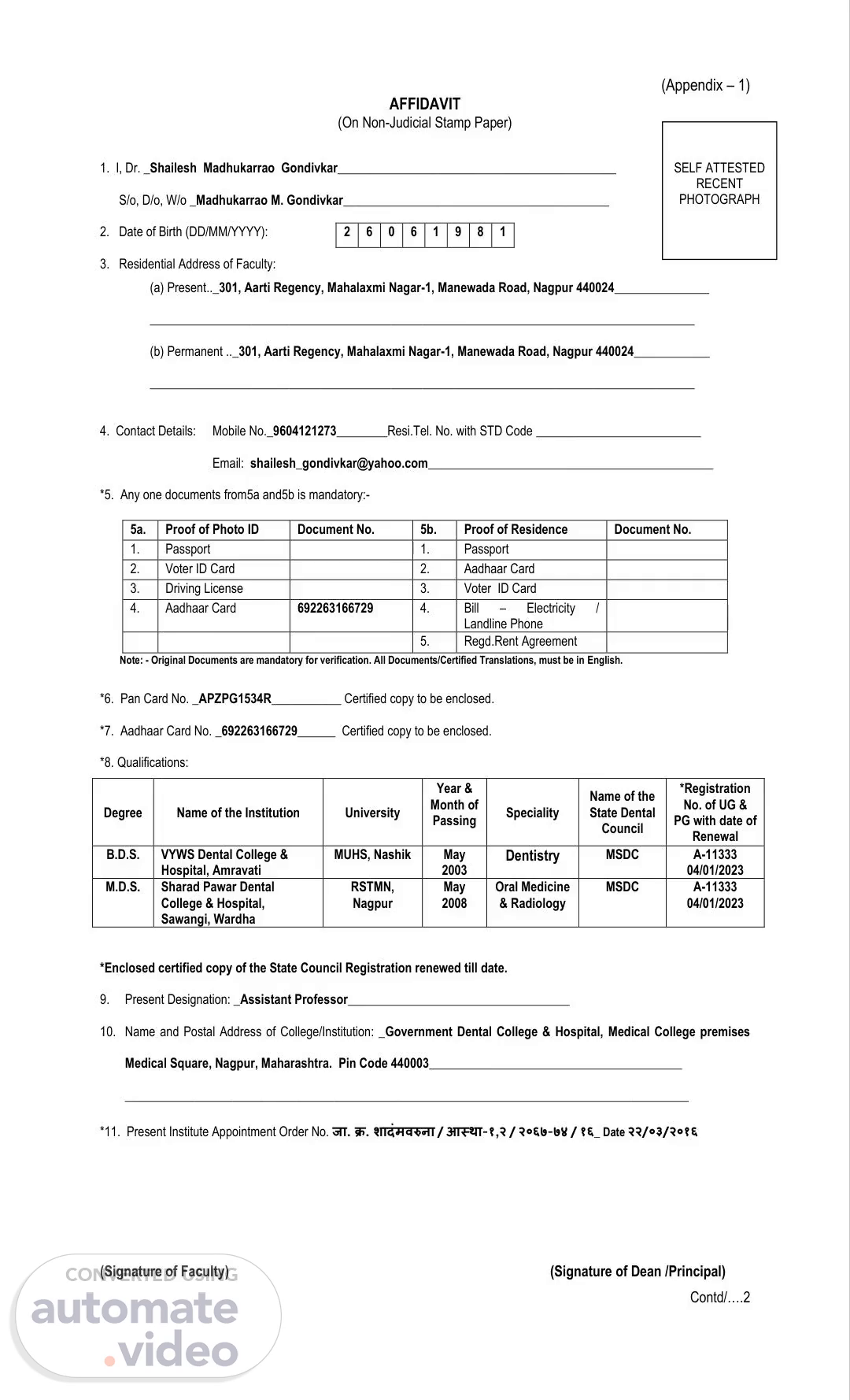
[Audio] (Appendix – 1) AFFIDAVIT (On Non-Judicial Stamp Paper) SELF ATTESTED RECENT PHOTOGRAPH 2 6 0 6 1 9 8 1 1. I, Dr. _Shailesh Madhukarrao Gondivkar____________________________________________ S/o, D/o, W/o _Madhukarrao M. Gondivkar__________________________________________ 2. Date of Birth (DD/MM/YYYY): 3. Residential Address of Faculty: (a) Present.._301, Aarti Regency, Mahalaxmi Nagar-1, Manewada Road, Nagpur 440024_______________ ______________________________________________________________________________________ (b) Permanent .._301, Aarti Regency, Mahalaxmi Nagar-1, Manewada Road, Nagpur 440024____________ ______________________________________________________________________________________ 4. Contact Details: Mobile No._9604121273________Resi.Tel. No. with STD Code __________________________ Email: [email protected]_____________________________________________ *5. Any one documents from5a and5b is mandatory:- 5a. Proof of Photo ID Document No. 5b. Proof of Residence Document No. 1. Passport 1. Passport 2. Voter ID Card 2. Aadhaar Card 3. Driving License 3. Voter ID Card 4. Aadhaar Card 692263166729 4. Bill – Electricity / Landline Phone 5. Regd.Rent Agreement Note: - Original Documents are mandatory for verification. All Documents/Certified Translations, must be in English. *6. Pan Card No. _APZPG1534R___________ Certified copy to be enclosed. *7. Aadhaar Card No. _692263166729______ Certified copy to be enclosed. *8. Qualifications: *Registration No. of UG & Degree Name of the Institution University Speciality Name of the State Dental Year & Month of Passing PG with date of Council Renewal B.D.S. VYWS Dental College & Hospital, Amravati MUHS, Nashik May 2003 Dentistry MSDC A-11333 04/01/2023 RSTMN, Nagpur May 2008 Oral Medicine & Radiology MSDC A-11333 04/01/2023 M.D.S. Sharad Pawar Dental College & Hospital, Sawangi, Wardha *Enclosed certified copy of the State Council Registration renewed till date. 9. Present Designation: _Assistant Professor___________________________________ 10. Name and Postal Address of College/Institution:.
Scene 2 (3m 40s)
[Audio] – 2 – *12. Before joining present institution I was working at MGV's KBH Dental College & Hospital, Nashik_____________ as _Reader____________________________and relieved on 21/03/2016___________after Resigning/Retiring. (i)Appointment Order No. _Ref. no. MGVN/MED/758/2012-13______& Date _02/06/2012 of the previous appointment: (ii) Relieving Order No. MGV/KBHDC/1487/2015-16__________ & Date_21/03/2016____________ *13. TEACHING EXPERIENCE* Position Name of Institution From To Total Experience 02/06/2008 13/09/2010 02 years 03 Lecturer/Asst. Professor KM Shah Dental College & Hospital, Waghodia, Vadodara months 14/09/2010 01/06/2012 01 year 08 Lecturer/Asst. Professor MGV's KBH Dental College & Hospital, Nashik months 02/06/2012 21/03/2016 03 years 09 Reader/Associate Professor MGV's KBH Dental College & Hospital, Nashik months 23/03/2016 Till date 07 years 09 Lecturer/Asst. Professor Government Dental College & Hospital, Nagpur months Dean/Principal * Less than one year teaching experience will not be considered.* Use separate box for each Institution. *14. TOTAL SALARY DRAWN FROM THE COLLEGE IN THE LAST SIX (6) MONTHS S.No. Month Amount Received Tax Deducted 1. JUL - 2023 131924 15000 2. AUG- 2023 117974 15000 3. SEP - 2023 117974 15000 4. OCT - 2023 117974 15000 5. NOV - 2023 131924 15000 6. DEC – 2023 (Last Six(6) months –Certified Copy of Bank Statement/Pass Book by the bank must be attached) *15. TDS FOR THE LAST THREE FINANCIAL YEARS: S.No. Financial Year TDS Paid 1. 2020-21 48940 2. 2021-22 71845 3. 2022-23 161655 (Copy of Form 16 generated from TRACES for last three financial years to be attached) *16. DETAILS OF PUBLICATIONS: S.No. Title of the Articles Journal Details Points J Oral Pathol Med. 2018 15 1. Bibliometric analysis of 100 most cited articles on oral submucous fibrosis Sep;47(8):781-787. Oral Diseases. 2023;29:873–879. 15 2. Heterogeneity of outcome measures in the clinical trials of treatment for oral submucous fibrosis—Systematic review 3. Assessment of oral health-related Oral Oncology 93 (2019) 39–45 15 quality of life instruments for oral submucous fibrosis: A systematic review using the COnsensus-based Standards for the selection of health Measurement Instruments (COSMIN) checklist Note: Submit certified clear Photocopies of all the documents mentioned in Serial No. 5, 6, 7, 8, 11,.
Scene 3 (8m 20s)
[Audio] – 3 – DECLARATION 1. I, Dr. _Shailesh M. Gondivkar____________________ do hereby give an undertaking that I am working as a full time salaried employee (as per UGC Norms) designated as _Assistant Professor_____________ in the Department of _Oral Medicine & Radiology at_Government Dental College & Hospital, Nagpur_____________________________ (name of the college) on all working days, working Hours from _8:30 AM_______ to _4:30 PM___________. 2. I am working as a Full Time/Part Time* faculty. (*As per Rule 16 of DCI, Master of Dental Surgery Course Regulations, 2017) 3. I have not presented myself to any other Institution as a faculty in the current academic year for the purpose of DCI Inspection. 4. I am not having private practice anywhere OR I am practicing at __________________________________ in the city of ____________________ and my days and hours of practice are ________________________ _____________________________________________________________________________________. 5. I, hereby, declare that the above information and documents provided by me are absolutely true, correct and authentic to the best of my knowledge. In the event of any statement made in this declaration is found to be incorrect or false I fully understand that I am liable for any necessary disciplinary/legal action. Date: (Signature of the Deponent) This is to certify that the information given by the above deponent is correct and nothing has been concealed and deponent is working in the _Oral Medicine & Radiology_____ (department) as __Assistant Professor____________ (designation) as a full-time teacher in our college and is not engaged in full-time private practice anywhere. Signature of Principal of the College Signature of the Chairman of the Trust with seal and date with seal and date Attestation by Notary Public/Oath Commissioner CERTIFIED THAT THE DEPONENT Dr. …………………………………………. S/o, W/o, D/o ………………..…………… Identified by Shri …………………………. has solemnly affirmed before me at …… on ………….…….. at Sl. No. …………… that the contents of the affidavit which have been read and explained to him/her are true and correct to his/her knowledge. Signature Notary Public/Oath Commissioner _____________________________________________________________________________________________________________________________________________________________ Counter Signature of the Deponent (On the day of Inspection) We have verified all the relevant documents and confirmed that information given are true to our knowledge and the above staff member was present during the inspection. (Signature of Inspector – 1) (Signature of Inspector – 2) Dr. _________________________________________ Dr. _________________________________________ Date ________________________ Date ________________________ [N.B. Please note that making false statement in the affidavit will attract the relevant.